Get the free billing hcfa 1500 form
Show details
Physician s/supplier s billing name address zip code and phone 24j Enter the total charge for this claim. This is the total of all charges for each service noted in Field services billed on this claim. any amount entered in Field 29. NOTE The person rendering care must sign and indicate licensure level. rendered. Not Form CMS-1500 08-05 as early as October 1 2006. NOTE The person rendering care must sign and indicate licensure level. rendered. Not Form CMS-1500 08-05 as early as October 1...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign hcfa form printable
Edit your printable medical claim form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your claim form instructions form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing cms 1500 forms printable online



Use the instructions below to start using our professional PDF editor:
1
Log into your account. If you don't have a profile yet, click Start Free Trial and sign up for one.
2
Upload a file. Select Add New on your Dashboard and upload a file from your device or import it from the cloud, online, or internal mail. Then click Edit.
3
Edit cms 1500 form. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Save your file. Select it in the list of your records. Then, move the cursor to the right toolbar and choose one of the available exporting methods: save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud.
It's easier to work with documents with pdfFiller than you can have believed. You may try it out for yourself by signing up for an account.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out download cms 1500 claim form
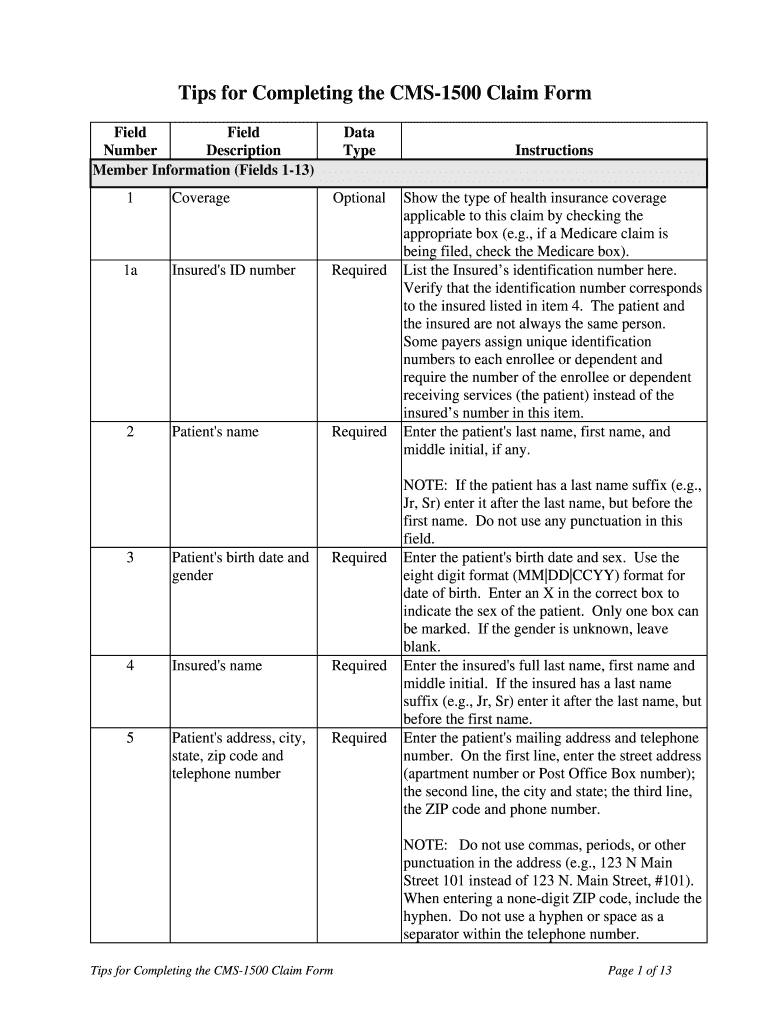
How to fill out Tips CMS-1500 Claim Form
01
Obtain a blank CMS-1500 claim form.
02
Fill out the patient’s details in Section 1 (Patient's Name, Address, and other identifying information).
03
Complete the insured's information in Section 2, if applicable.
04
In Section 3, write the patient's birth date and gender.
05
Indicate the type of insurance coverage in Section 4 (e.g., Medicare, Medicaid).
06
In Section 5, provide the provider's information (name, NPI number, address).
07
Fill in Section 6 with the patient’s relationship to the insured.
08
In Section 7, specify the ICD diagnosis codes.
09
Complete Section 8 with the date of the injury or illness, if relevant.
10
In Section 9, include any relevant billing information (i.e., claim-related comments).
11
Fill in Section 10 with pertinent additional information, if needed.
12
In Section 11, list the services provided, including dates, procedure codes, and charges.
13
Verify the accuracy of the information, ensure that all required fields are filled out, then sign and date the form.
Who needs Tips CMS-1500 Claim Form?
01
Healthcare providers billing for medical services rendered.
02
Insurance companies processing claims for reimbursement.
03
Patients needing to submit claims for covered services to their insurer.
04
Medical billers responsible for managing claims on behalf of providers.
Fill
cms 1500 billing instructions
: Try Risk Free
People Also Ask about hcfa 1500 form
What is the difference between HCFA-1500 and CMS 1500?
What is a CMS-1500? Also referred to as the HCFA or the 1500, this form was developed by NUCC as the standard form for individual doctors, nurses, practices and other professionals. This form can also list prior payer information when being sent to secondary, though this is not always utilized.
What is a CMS 1500 form used for?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
How to fill out a CMS 1500 claim form?
How to fill out a CMS-1500 form The type of insurance and the insured's ID number. The patient's full name. The patient's date of birth. The insured's full name, if applicable. The patient's address. The patient's relationship to the insured, if applicable. The insured's address, if applicable. Field reserved for NUCC use.
Is CMS 1500 same as UB04?
While the CMS-1500 and UB-04 forms may look similar, they are very different and have distinct purposes. Thus, the two forms cannot be used interchangeably.
What is CMS 1500 claim form?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
What is CMS 1500 or ub04 form?
The UB-04 (CMS-1450) form is the claim form for institutional facilities such as hospitals or outpatient facilities. This would include things like surgery, radiology, laboratory, or other facility services. The HCFA-1500 form (CMS-1500) is used to submit charges covered under Medicare Part B.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I complete cms 1500 pdf online?
pdfFiller makes it easy to finish and sign cms 1500 claim form online. It lets you make changes to original PDF content, highlight, black out, erase, and write text anywhere on a page, legally eSign your form, and more, all from one place. Create a free account and use the web to keep track of professional documents.
How can I edit cms 1500 claim form instructions on a smartphone?
You may do so effortlessly with pdfFiller's iOS and Android apps, which are available in the Apple Store and Google Play Store, respectively. You may also obtain the program from our website: https://edit-pdf-ios-android.pdffiller.com/. Open the application, sign in, and begin editing cms 1500 modifier codes right away.
How do I fill out cms 1500 instructions for beginners using my mobile device?
The pdfFiller mobile app makes it simple to design and fill out legal paperwork. Complete and sign form cms 1500 cheat sheet and other papers using the app. Visit pdfFiller's website to learn more about the PDF editor's features.
What is Tips CMS-1500 Claim Form?
The CMS-1500 Claim Form is a standardized form used by healthcare providers to bill Medicare and Medicaid, as well as private insurance companies, for services rendered to patients.
Who is required to file Tips CMS-1500 Claim Form?
Healthcare providers, including physicians, therapists, and other professionals who provide medical services and wish to seek payment from insurance companies, are required to file the CMS-1500 Claim Form.
How to fill out Tips CMS-1500 Claim Form?
To fill out the CMS-1500 Claim Form, providers must enter patient information, insurance details, services provided, diagnosis codes, and other necessary information accurately in the designated fields, following specific guidelines.
What is the purpose of Tips CMS-1500 Claim Form?
The purpose of the CMS-1500 Claim Form is to facilitate the billing process by providing a structured way for healthcare providers to request payment for services rendered from insurance payers.
What information must be reported on Tips CMS-1500 Claim Form?
The CMS-1500 Claim Form must include information such as the patient's name, address, date of birth, insurance policy number, provider's National Provider Identifier (NPI), service dates, procedure codes, diagnosis codes, and total charges.
Fill out your billing hcfa 1500 form online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
1500 Form Pdf is not the form you're looking for?Search for another form here.
Keywords relevant to physician billing form 1500
Related to hcfa pdf fillable



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
