Last updated on Jun 20, 2026
Get the free CMS-1500 Claim Form
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is CMS-1500 Claim Form
The CMS-1500 Claim Form is a health insurance claim form used by patients and insured individuals to submit medical claims to health insurance providers in the United States.
pdfFiller scores top ratings on review platforms
Who needs CMS-1500 Claim Form?
Explore how professionals across industries use pdfFiller.

CMS-1500 Claim Form is needed by:
-
Patients seeking reimbursement for medical services.
-
Insured individuals needing to file claims with their insurance provider.
-
Healthcare providers completing claims on behalf of patients.
-
Insurance companies reviewing submitted claims.
-
Billing departments in healthcare facilities managing claims processing.
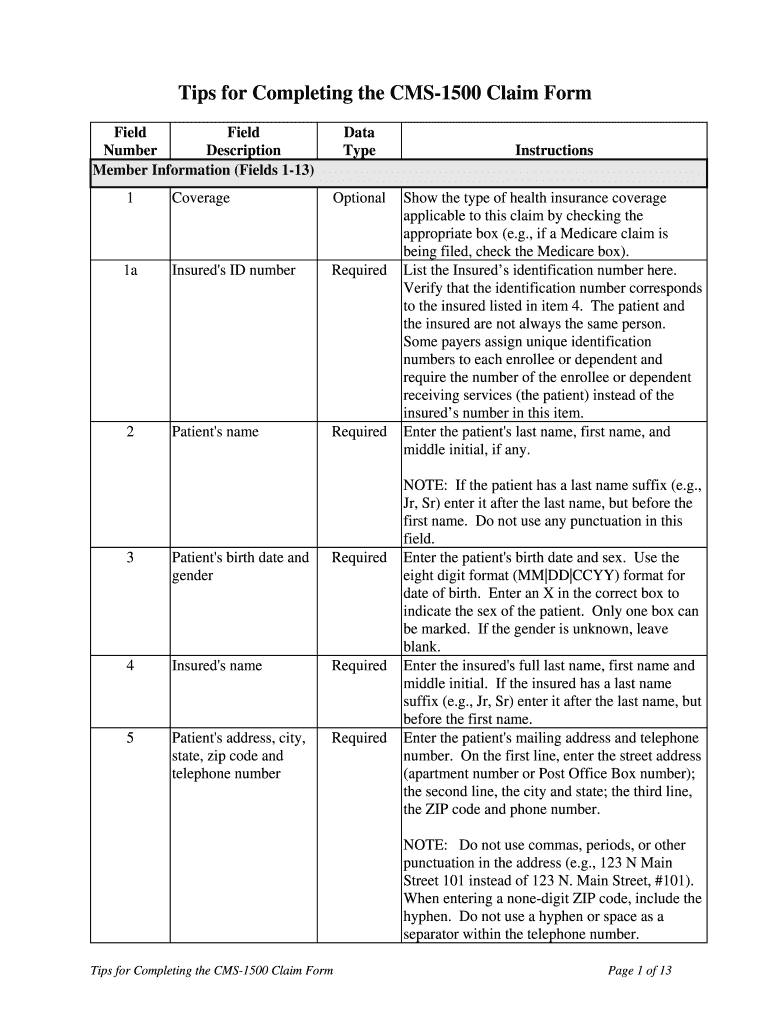
Comprehensive Guide to CMS-1500 Claim Form
Understanding the CMS-1500 Claim Form
The CMS-1500 Claim Form serves as a crucial health insurance claim form utilized across the United States. It is essential for efficiently communicating claim details to health insurance providers. Accurate completion of this form plays a vital role in ensuring prompt claim processing, ultimately impacting reimbursement timelines for healthcare services.
This form is paramount in medical billing, streamlining the insurance claims process by providing necessary patient and service information. Understanding its components helps both patients and healthcare providers navigate insurance requirements more effectively.
Why You Need the CMS-1500 Claim Form
The CMS-1500 Claim Form is essential for various stakeholders within the healthcare ecosystem. Patients and insured individuals rely on this form to facilitate their claims, while healthcare providers use it to ensure they receive timely payments for their services. The benefits of utilizing this form significantly enhance the efficiency of reimbursement processes.
Common scenarios necessitating the form’s use include office visits, diagnostic tests, and treatment procedures. Its importance cannot be overstated, as it helps avoid delays due to improper submissions.
Key Features of the CMS-1500 Claim Form
The CMS-1500 Claim Form contains several essential components designed to capture detailed information. Each section is tailored for specific entries:
-
Patient information, including demographics and insurance details
-
Insured information, ensuring proper claim linkage
-
Provider information, identifying the healthcare professional or facility rendering services
Understanding the purpose of checkboxes and the context of each section can significantly enhance the accuracy of submissions. Properly completing each part reduces the likelihood of processing issues.
Who Is Required to Sign the CMS-1500 Claim Form?
Two primary roles require signatures on the CMS-1500 Claim Form: the 'Patient' and the 'Insured.' It is crucial to gather signatures from both parties to validate the authenticity of the claim.
Lack of required signatures can lead to delays or rejection of the claim, underscoring the need for compliance with these requirements for both legal and processing purposes. Understanding the responsibilities attached to each role simplifies the process.
How to Fill Out the CMS-1500 Claim Form Online (Step-by-Step)
Filling out the CMS-1500 Claim Form digitally can simplify the submission process. Here is a step-by-step guide to effectively complete the form:
-
Please enter patient and insured information in the designated fields.
-
Provide accurate medical service details, including dates and descriptions.
-
Double-check for completeness and accuracy before finalizing submissions.
Common pitfalls include missing signatures and incorrect data entries. Being aware of these mistakes and adopting a thorough review process enhances the likelihood of successful claim processing.
Submitting the CMS-1500 Claim Form: Methods & Best Practices
Submitting the completed CMS-1500 Claim Form can be done through various methods. Healthcare providers often choose between mailing the form or opting for electronic submission. Each method has its advantages and potential drawbacks.
To ensure the best outcomes when filing claims, consider the following best practices:
-
Ensure all fields are completed accurately before submission.
-
Utilize electronic submission for faster processing times when possible.
-
Keep a record of submissions to track and confirm receipt.
Common Errors in the CMS-1500 Claim Form and How to Avoid Them
Awareness of frequent errors when completing the CMS-1500 Claim Form can greatly reduce claim processing delays. Some common mistakes include:
-
Entering incorrect patient or provider information
-
Missing necessary signatures from patients or the insured
-
Omitting key service details or dates
Ensuring accuracy is vital, as incorrect information can have severe implications for claim approval. A checklist can help verify entries before submission to minimize these errors.
The Role of pdfFiller in Completing the CMS-1500 Claim Form
pdfFiller significantly simplifies the process of filling out the CMS-1500 Claim Form with features designed for ease of use. The platform allows users to access templates that facilitate eSigning and editing directly within the document.
Utilizing pdfFiller enhances security and compliance while managing sensitive healthcare documents. User testimonials highlight the benefits of its user-friendly interface, demonstrating how it aids in streamlining the healthcare billing process.
What Happens After You Submit the CMS-1500 Claim Form?
Once the CMS-1500 Claim Form is submitted, a systematic processing timeline begins. Typically, healthcare providers can expect a specific period during which claims are evaluated and processed.
Tracking the status of your claim is crucial. Healthcare providers should be aware of the next steps, which include addressing any rejections promptly or providing additional information if requested.
Get Started with the CMS-1500 Claim Form Today
Using pdfFiller, you can access the CMS-1500 Claim Form easily to streamline your healthcare billing process. The easy fillable forms empower you to submit medical claims efficiently.
With robust security features and a user-friendly interface, pdfFiller offers an effective solution for navigating the complexities associated with healthcare billing.
How to fill out the CMS-1500 Claim Form
-
1.To access the CMS-1500 Claim Form on pdfFiller, visit the website and search for the form using the search bar. Select the correct version from the search results.
-
2.Once you have opened the form, you can navigate through the blank fields using your mouse or keyboard. Click into each field to begin entering data.
-
3.Before filling out the form, gather all necessary information including patient details, insured information, service dates, medical procedures, and provider contact information.
-
4.As you fill in the CMS-1500 form, ensure that you follow the instructions provided for each section. Fill in patient and insured information accurately to avoid processing delays.
-
5.Review all entered information for accuracy and completeness, checking for any missing fields or incorrect entries.
-
6.Once you have completed the form, check the preview to see how it looks. Make any necessary edits to ensure clarity and correctness.
-
7.To save your completed form, click the save button on pdfFiller. You can also download a copy to your device or submit the form electronically if that option is available.

Who is eligible to use the CMS-1500 Claim Form?
The CMS-1500 Claim Form is designed for patients and insured individuals looking to submit claims for medical services. Both parties must ensure they have complete and accurate information to use the form effectively.
What supporting documents are required when submitting the CMS-1500 form?
When submitting the CMS-1500 Claim Form, ensure to include any necessary supporting documentation, such as itemized bills, medical records, or proof of insurance, to avoid delays in processing.
How can I submit the CMS-1500 Claim Form?
The CMS-1500 Claim Form can typically be submitted electronically through your health insurance provider's online portal or by mailing it to the address specified by your insurer. Always confirm submission methods with your insurance company.
Are there any common mistakes to avoid when filling out the CMS-1500 form?
Common mistakes include leaving required fields blank, using outdated information, and failing to sign the form where necessary. Double-checking for accuracy before submission can help prevent these issues.
What is the processing time for claims submitted using the CMS-1500 form?
Processing times for claims submitted via the CMS-1500 form can vary by insurance provider, but typically it takes between 14 to 30 days. It's advisable to follow up with your insurer if there are delays.
Is there a deadline for submitting the CMS-1500 Claim Form?
Yes, most insurance providers have specific deadlines for submitting claims, usually ranging from 30 to 180 days after the service date. Confirm with your insurer to ensure timely submission.
Can I fill out the CMS-1500 Claim Form online?
Yes, you can fill out the CMS-1500 Claim Form online using platforms like pdfFiller, which provides tools for easy completion and electronic submission of the form.
Related Content
Related Forms



Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.